Have you ever filled a prescription and been shocked by the price - only to find out there’s no cheaper generic version available? It’s not a glitch. It’s not bad luck. It’s the system working exactly as designed - for pharmaceutical companies, not patients.
Not all brand-name drugs have generic versions, even after years on the market. Some, like EpiPen, Spiriva, or Humira, still cost hundreds or even thousands of dollars per month, decades after they were first approved. Meanwhile, drugs like Lipitor or Nexium dropped to a fraction of their original price as soon as generics arrived. So why do some drugs stay expensive forever?
Patents aren’t the whole story
The simplest answer is patents. When a drug company invents a new medicine, it gets a 20-year patent. That’s the legal monopoly that lets them charge high prices to recoup research costs. Once the patent expires, generics can enter the market - or so you’d think.
But here’s the catch: patents are just the starting point. Drugmakers use legal tricks to stretch that monopoly. They file for additional patents on things like the pill’s coating, the way it’s swallowed, or even the shape of the tablet. These aren’t new inventions - they’re tiny tweaks. But under U.S. law, each one can add another year or two of exclusivity. This is called patent thickets. One drug might have 50+ patents listed in the FDA’s Orange Book, and most of them have nothing to do with how the drug works - they’re just barriers to keep generics out.
Take Nexium. The original drug, Prilosec, lost its patent in 2001. But AstraZeneca quickly launched Nexium - a slightly modified version of the same active ingredient - and got a new 20-year patent. By the time Nexium’s patent expired in 2014, the company had made billions. This tactic, called product hopping, delays generics by years.
Some drugs can’t be copied - not even if they wanted to
Not all drugs are made the same way. Simple pills with one chemical compound - like atorvastatin for cholesterol - are easy to copy. But some drugs are made from living cells, complex mixtures, or natural sources that can’t be perfectly replicated.
Premarin, a hormone therapy for menopause, is made from the urine of pregnant mares. It contains a mix of 10+ different estrogen compounds, many of which aren’t fully identified. No generic company can guarantee they’re copying the exact same blend. The FDA won’t approve a copy unless it’s identical - and with Premarin, that’s scientifically impossible.
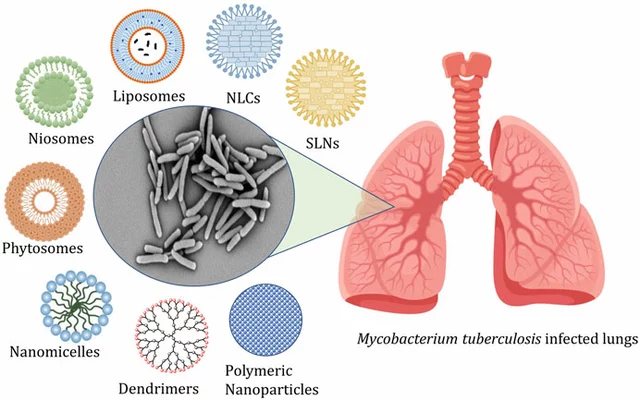
Biologics are another category. These are large, complex molecules made from living organisms - like Humira for rheumatoid arthritis or Enbrel for psoriasis. You can’t just mix chemicals in a lab to make them. You need living cells, precise growing conditions, and advanced purification. That’s why generics for these drugs are called biosimilars, not generics. And biosimilars require 12 years of exclusivity before they can even be considered - far longer than the 5 years for regular generics. The first biosimilar for Humira didn’t hit the U.S. market until 2023, even though the patent expired in 2016.
The FDA’s high bar for approval
Even when a drug is simple enough to copy, the FDA demands proof that the generic works the same way. For most pills, that means showing the body absorbs the same amount of the drug within a narrow range - 80% to 125% of the brand-name version.
But for drugs with a narrow therapeutic index, that margin is too wide. Think epilepsy meds like phenytoin or thyroid drugs like levothyroxine. If the generic absorbs even 5% differently, it could trigger seizures or cause heart problems. The FDA requires extra testing - sometimes clinical trials - to prove safety. That adds years and millions of dollars to the approval process.
Complex delivery systems also slow things down. Inhalers like Advair, patches like Androderm, or extended-release capsules like Prozac Weekly aren’t just about the active ingredient. The way the drug is released into your body matters. A generic manufacturer has to reverse-engineer the entire delivery system - the polymers, the coatings, the slow-release beads - without knowing the exact formula. It’s like trying to copy a watch without seeing the inside.
Companies pay generics to stay away
Here’s the dirtiest trick: pay-for-delay. Sometimes, the brand-name company doesn’t fight in court. Instead, they pay the generic manufacturer to hold off. In exchange for millions of dollars, the generic company agrees not to launch its version for years.
The Federal Trade Commission found 297 of these deals between 1999 and 2012. One deal paid a generic maker $1.2 billion to delay a generic version of the antidepressant Wellbutrin for six years. These agreements cost consumers an estimated $3.5 billion every year in higher drug prices.
It’s legal - for now. But the CREATES Act of 2019 made it harder for brand-name companies to block generic makers from getting samples of the drug they need to test. Still, many pay-for-delay deals are still active, especially for high-revenue drugs.
Why the cost difference matters
The price gap isn’t small. A 2022 GoodRx analysis found that brand-name drugs without generics cost, on average, 437% more than those with generic alternatives. For patients on Medicare Part D, 22% of those taking non-generic drugs spend over $5,000 a year out of pocket. That’s more than many people pay for rent.
Compare that to Lipitor. When its patent expired in 2011, dozens of generic makers entered the market. Within a year, the price dropped 85%. A 30-day supply went from $180 to under $15. That’s the power of competition.
But for drugs like Gleevec, used to treat leukemia, patients paid $14,500 a month before the generic arrived in 2016. After? $850. One patient on Reddit said the generic saved their life - not because it worked better, but because they could actually afford it.

What patients can do
If your drug has no generic, you’re not stuck. Talk to your doctor. Ask if there’s a similar drug that’s already generic. For example, if Viibryd (vilazodone) is too expensive, sertraline or escitalopram might work just as well for depression - and cost a fraction.
Pharmacists can help too. They track patent expirations and know when a biosimilar is coming. Ask them if there’s a therapeutic alternative you haven’t considered.
Check the FDA’s Orange Book. It lists every patent and exclusivity period for branded drugs. You can search by name and see when a generic might arrive - even if it’s years away.
And don’t assume the brand-name version is better. For 90% of drugs, generics are identical in safety and effectiveness. The only difference? The price tag.
The future: More generics, but not all
The FDA is speeding up reviews for complex generics. In 2022, approvals for these harder-to-copy drugs rose 27% compared to 2021. Biosimilars are growing fast - from 32 in 2022 to an expected 75 by 2025.
But experts agree: about 5% of drugs will never have true generics. These are the ultra-complex biologics, orphan drugs for rare diseases, and formulations with impossible-to-replicate delivery systems. Insulin, for example, still has no true generic - only biosimilars - and won’t until at least 2026.
That means for some patients, high drug costs aren’t temporary. They’re permanent. And until the system changes, those patients will keep paying the price for innovation - while others get to save.